
Best PRP System: 3 qualities to check and a comparison of different PRP systems
Not all PRP is the same
Platelet-rich plasma, or PRP, is simply plasma (the fluid that flows through your blood vessels), with a high concentration of autologous platelets. According to the classic definition of PRP, the minimum concentration for PRP should be 1 million platelets per microlitre.1 See this post for more basic information about PRP.
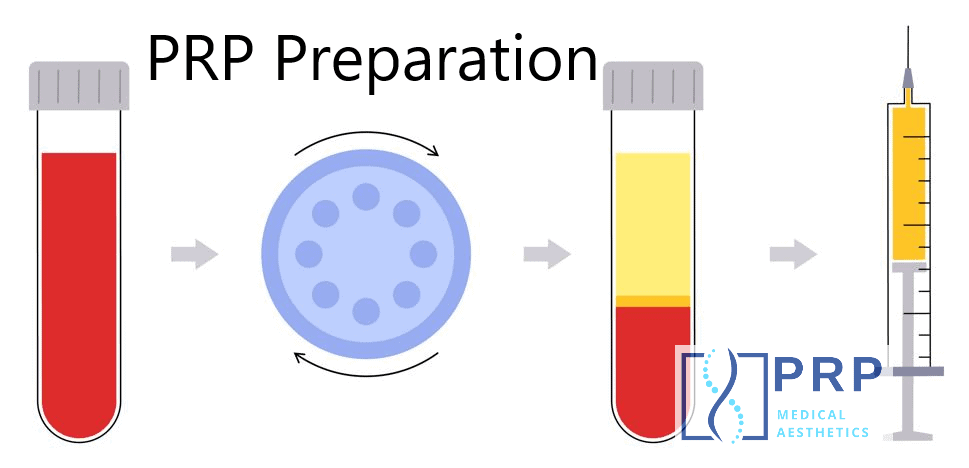
The concept is actually quite simple. Preparation of autologous platelet rich plasma starts with sample of blood. Almost all preparation methods will use a centrifuge to separate the blood into three different layers: red blood cells (RBCs), buffy coat, and plasma. Often, after this first step, the plasma is already called PRP, (or sometimes PRF, platelet-rich fibrin, more on this later). Other times, the preparation time is extended, taking the plasma into a double-spin process, which can generally yield a higher concentration for PRP.
Why PRP kits fail: Different Quality, Concentration, Purity, and Dose
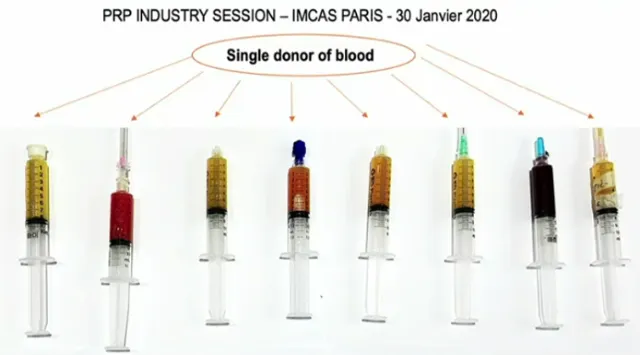
The most important thing to know about PRP is that not all PRP is the same. There are large differences in terms of platelet concentration, purity (cellular composition), and platelet dose2. In simple terms, ideal PRP has three important things:
Best PRP System – 3 Characteristics of Ideal PRP:
- High concentration (over 1 million platelets/µL)
- High purity (over 90% pure platelets, less than 10% RBCs & WBCs)
- Proper dose (usually 4-6 billion platelets total)
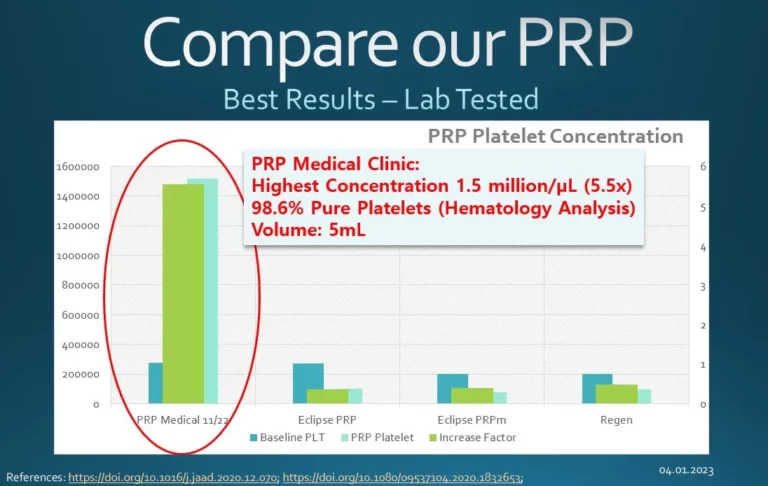
1. PRP High Platelet Concentration (goal > 1 million/uL)
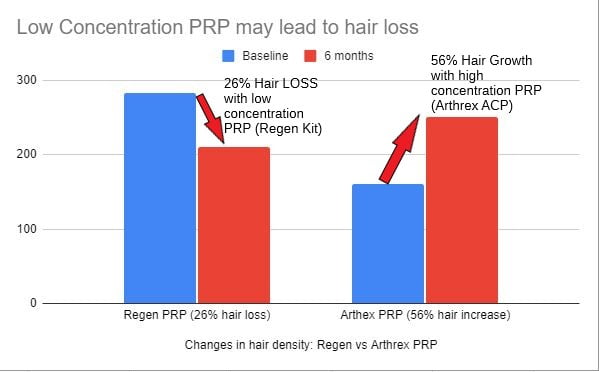
Platelet concentration (/uL) of different PRP systems has been shown in studies to be as little as 80 thousand to over 2 million. That’s over 2500% difference, which is astounding. It means far fewer growth factors in the less concentrated PRP. Why does it matter? One study showed that low platelet concentration PRP was associated with more HAIR LOSS after PRP. In our testing, we have analyzed PRP from other clinics that had platelet concentration as low as 4 thousand, which is 98% lower than whole blood, and 250x lower than the 1 million target concentration.
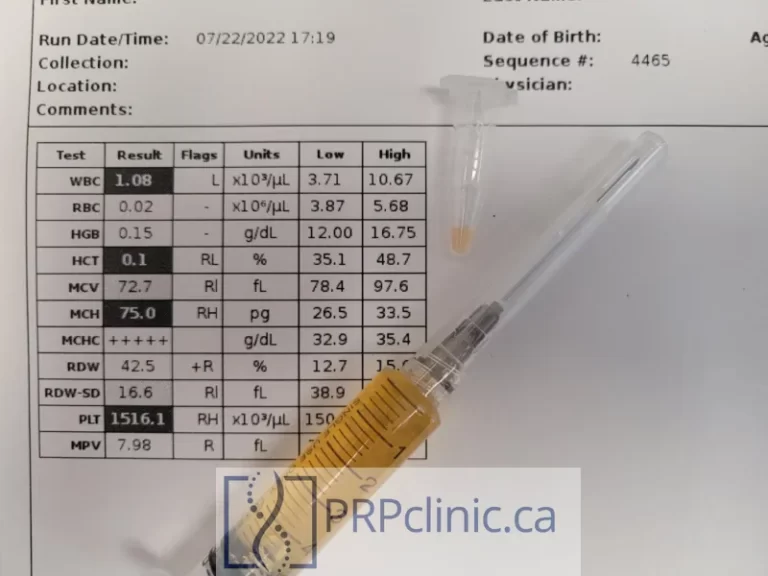
2. PRP High Purity (goal > 95%)
PRP purity is simple the percentage of cells in the plasma that are platelets compared to red blood cells (RBCs) or white blood cells (leukocytes, or WBCs). If 90% of the cells are platelets, the PRP is considered 90% pure.
IMPORTANT: High purity without high concentration is useless and may actually be harmful (e.g. associated with hair loss). For example, some PRP kits produce over 99% purity, but the overall platelet concentration is so low, the growth factor concentration would be extremely low.
3. PRP High Dose (goal ~5 billion, depending on treatment)
Having PRP that is high in concentration and purity is great, but the final question is how much of that is available for a single treatment? Is it a few drops, or a few mL? This is important for clinical effect. For example, if we’re doing a scalp treatment (PRP for Hair Loss), ideally we’d want to have 6 mL of PRP with a concentration of 1 million/uL or more. This would give a final DOSE of 6 billion platelets.
PRP Comparison Table (concentration, purity, dose)
Here’s a concentration table of the various PRP systems that have been tested in the scientific literature, including PRP that we have produced and analyzed at our clinic. You may notice that several systems have been tested more than once, and the results are not always the same. This is an important fact: PRP systems vary widely, even the same system will give different results from the same blood and we don’t really know why. This is why it’s so important to test PRP every time.
| PRP Name | Reference | Region | Single /Double | PRP Platelet X Factor | PRP Platelet Concentration (x1000, baseline 225k/uL) | PRP Concentration Rating | PRP Platelet Purity (Goal > 95%) | PRP Purity Rating | PRP Volume | PRP Platelet Dose (billions) | PRP Dose Rating | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| "Perfect PRP (in theory)" | North America | Double | 5.0 | 1125 | ⭐⭐⭐⭐⭐ | HC | 96.0 | ⭐⭐⭐⭐⭐ | yes | 6 | 6.75 | ⭐⭐⭐⭐ | yes | |||
| Eclipse | Mandle 2015 | https://accelleratedbiologics.com/assets/casestudies/accell-casestudy-comparison-%20emcyte-prp.pdf | gel tube | North America | Single | 0.4 | 90 | ☆VERY LOW | 99.6 | ⭐⭐⭐⭐⭐ | yes | 6 | 0.54 | ☆VERY LOW | no | |
| Regen | Mandle 2015 | https://accelleratedbiologics.com/assets/casestudies/accell-casestudy-comparison-%20emcyte-prp.pdf | gel tube | North America | Single | 0.5 | 113 | ☆VERY LOW | 99.2 | ⭐⭐⭐⭐⭐ | yes | 6 | 0.68 | ☆VERY LOW | no | |
| Curasan | Kaux 2009 | https://pubmed.ncbi.nlm.nih.gov/19481375/ | non-gel tube | Europe | 2.8 | 630 | ⭐⭐⭐ | 97.7 | ⭐⭐⭐⭐⭐ | yes | 1 | 0.63 | ☆VERY LOW | no | ||
| Regen | Kaux 2009 | https://pubmed.ncbi.nlm.nih.gov/19481375/ | gel tube | North America | Single | 1.6 | 360 | ⭐ | 97.5 | ⭐⭐⭐⭐⭐ | yes | 3.1 | 1.12 | ☆VERY LOW | no | |
| FIDIA Hy-tissue 20 | Degen 2017 | https://pubmed.ncbi.nlm.nih.gov/28167878/ | non-gel tube | Europe | Single | 1.4 | 315 | ⭐ | 96.6 | ⭐⭐⭐⭐⭐ | yes | 8.8 | 2.77 | ⭐ | no | |
| ARTHREX ACP | Fitzpatrick 2017 | https://pubmed.ncbi.nlm.nih.gov/28210651/ | automated device | North America | 1.5 | 338 | ⭐ | 92.3 | ⭐⭐⭐⭐ | yes | 6.5 | 2.19 | ⭐ | no | ||
| ARTHREX Angel 2% HCT | Degen 2017 | https://pubmed.ncbi.nlm.nih.gov/28167878/ | automated device | North America | 10.0 | 2250 | ⭐⭐⭐⭐⭐ | HC | 90.7 | ⭐⭐⭐⭐ | yes | 2.9 | 6.53 | ⭐⭐⭐⭐ | yes | |
| Regen | Atashi 2015 | https://pubmed.ncbi.nlm.nih.gov/25025830/ | gel tube | North America | Single | 1.7 | 383 | ⭐ | 88.7 | ⭐⭐⭐ | 4 | 1.53 | ☆VERY LOW | no | ||
| ARTHREX ACP | Oh 2015 | https://pubmed.ncbi.nlm.nih.gov/26473014/ | automated device | North America | 2.4 | 540 | ⭐⭐ | 87.7 | ⭐⭐⭐ | 3 | 1.62 | ☆VERY LOW | no | |||
| Plateltex | Kaux 2009 | https://pubmed.ncbi.nlm.nih.gov/19481375/ | non-gel tube | Europe | Single | 3.4 | 765 | ⭐⭐⭐ | 87.5 | ⭐⭐⭐ | 0.3 | 0.23 | ☆VERY LOW | no | ||
| MTF Cascade | Castillo 2011 | https://pubmed.ncbi.nlm.nih.gov/21051428/ | gel tube | Europe | Single | 1.6 | 360 | ⭐ | 81.4 | ⭐⭐ | 7.5 | 2.70 | ⭐ | no | ||
| ARTHREX ACP | Magalon 2014 | https://pubmed.ncbi.nlm.nih.gov/24725317/ | automated device | North America | 1.3 | 293 | ⭐ | 81.0 | ⭐⭐ | 4 | 1.17 | ☆VERY LOW | no | |||
| PRODIZEN Prosys | Oh 2015 | https://pubmed.ncbi.nlm.nih.gov/26473014/ | transfer to secondary disposable | Europe | Double | 4.2 | 945 | ⭐⭐⭐⭐ | HC | 79.2 | ⭐⭐ | 3 | 2.84 | ⭐ | no | |
| SELPHYL | Magalon 2014 | https://pubmed.ncbi.nlm.nih.gov/24725317/ | gel tube | North America | Single | 1.2 | 270 | ⭐ | 73.9 | ⭐⭐ | 4.1 | 1.11 | ☆VERY LOW | no | ||
| ARTHREX Angel 7% HCT | Degen 2017 | https://pubmed.ncbi.nlm.nih.gov/28167878/ | automated device | North America | 11.2 | 2520 | ⭐⭐⭐⭐⭐ | HC | 69.4 | ⭐⭐ | 3.5 | 8.82 | ⭐⭐⭐⭐⭐ | yes | ||
| ARTHREX ACP | Mazzocca 2012 | https://pubmed.ncbi.nlm.nih.gov/22336969/ | automated device | North America | 2.7 | 608 | ⭐⭐⭐ | 65.3 | ⭐⭐ | 3 | 1.82 | ☆VERY LOW | no | |||
| ARTERIOCYTE Magellan | Degen 2017 | https://pubmed.ncbi.nlm.nih.gov/28167878/ | automated device | North America | 9.7 | 2183 | ⭐⭐⭐⭐⭐ | HC | 64.0 | ⭐ | 5.3 | 11.57 | ⭐⭐⭐⭐⭐ | yes | ||
| EMCYTE GS30-Pure II | Mandle 2015 | https://accelleratedbiologics.com/assets/casestudies/accell-casestudy-comparison-%20emcyte-prp.pdf | transfer to secondary disposable | North America | Double | 5.4 | 1215 | ⭐⭐⭐⭐⭐ | HC | 63.9 | ⭐ | 4 | 4.86 | ⭐⭐⭐ | yes | |
| ARTERYOCYTE Magellan | Castillo 2011 | https://pubmed.ncbi.nlm.nih.gov/21051428/ | automated device | North America | 2.8 | 630 | ⭐⭐⭐ | 60.4 | ⭐ | 6 | 3.78 | ⭐⭐ | no | |||
| BIOMET GPS III | Degen 2017 | https://pubmed.ncbi.nlm.nih.gov/28167878/ | transfer to secondary disposable | Europe | Double | 6.5 | 1463 | ⭐⭐⭐⭐⭐ | HC | 56.7 | ⭐ | 6.1 | 8.92 | ⭐⭐⭐⭐⭐ | yes | |
| 3I PCCS | Leitner 2006 | https://pubmed.ncbi.nlm.nih.gov/16907874/ | Europe | 4.6 | 1035 | ⭐⭐⭐⭐⭐ | HC | 55.8 | ⭐ | 8.5 | 8.80 | ⭐⭐⭐⭐⭐ | yes | |||
| ARTERIOCYTE Magellan | Fitzpatrick 2017 | https://pubmed.ncbi.nlm.nih.gov/28210651/ | automated device | North America | 4.7 | 1058 | ⭐⭐⭐⭐⭐ | HC | 54.4 | ⭐ | 6.5 | 6.87 | ⭐⭐⭐⭐ | yes | ||
| BIOMET GPS | Eppley 2004 | https://pubmed.ncbi.nlm.nih.gov/15509939/ | transfer to secondary disposable | Europe | Double | 8.0 | 1800 | ⭐⭐⭐⭐⭐ | HC | 52.8 | ⭐ | 6 | 10.80 | ⭐⭐⭐⭐⭐ | yes | |
| BIOMET Mini GPS III | Magalon 2014 | https://pubmed.ncbi.nlm.nih.gov/24725317/ | transfer to secondary disposable | Europe | Double | 3.9 | 878 | ⭐⭐⭐⭐ | HC | 51.8 | ⭐ | 3.2 | 2.81 | ⭐ | no | |
| ARTERIOCYTE Magellan | Mandle 2015 | https://accelleratedbiologics.com/assets/casestudies/accell-casestudy-comparison-%20emcyte-prp.pdf | automated device | North America | 4.9 | 1103 | ⭐⭐⭐⭐⭐ | HC | 51.6 | ⭐ | 7 | 7.72 | ⭐⭐⭐⭐⭐ | yes | ||
| BIOMET GPS III | Oh 2015 | https://pubmed.ncbi.nlm.nih.gov/26473014/ | transfer to secondary disposable | Europe | Double | 7.3 | 1643 | ⭐⭐⭐⭐⭐ | HC | 51.0 | ⭐ | 6 | 9.86 | ⭐⭐⭐⭐⭐ | yes | |
| BIOMET GPS III | Fitzpatrick 2017 | https://pubmed.ncbi.nlm.nih.gov/28210651/ | transfer to secondary disposable | Europe | Double | 3.6 | 810 | ⭐⭐⭐⭐ | HC | 47.5 | ⭐ | 6.5 | 5.27 | ⭐⭐⭐ | yes | |
| HARVEST SmartPReP | Leitner 2006 | https://pubmed.ncbi.nlm.nih.gov/16907874/ | transfer to secondary disposable | North America | Double | 3.8 | 855 | ⭐⭐⭐⭐ | HC | 46.3 | ⭐ | 10 | 8.55 | ⭐⭐⭐⭐⭐ | yes | |
| BIOMET GPS III | Mazzocca 2012 | https://pubmed.ncbi.nlm.nih.gov/22336969/ | transfer to secondary disposable | Europe | Double | 6.1 | 1373 | ⭐⭐⭐⭐⭐ | HC | 46.1 | ⭐ | 3 | 4.12 | ⭐⭐ | no | |
| Regen | Magalon 2014 | https://pubmed.ncbi.nlm.nih.gov/24725317/ | gel tube | North America | Single | 1.6 | 360 | ⭐ | 46.0 | ⭐ | 3.1 | 1.12 | ☆VERY LOW | no | ||
| HARVEST SmartPReP 2 | Fitzpatrick 2017 | https://pubmed.ncbi.nlm.nih.gov/28210651/ | transfer to secondary disposable | North America | Double | 4.6 | 1035 | ⭐⭐⭐⭐⭐ | HC | 45.7 | ⭐ | 6.5 | 6.73 | ⭐⭐⭐⭐ | yes | |
| EMCYTE GS60-Pure II | Mandle 2015 | https://accelleratedbiologics.com/assets/casestudies/accell-casestudy-comparison-%20emcyte-prp.pdf | transfer to secondary disposable | North America | Double | 5.8 | 1305 | ⭐⭐⭐⭐⭐ | HC | 37.8 | ⭐ | 7 | 9.14 | ⭐⭐⭐⭐⭐ | yes | |
| HARVEST SmartPReP | Degen 2017 | https://pubmed.ncbi.nlm.nih.gov/28167878/ | transfer to secondary disposable | North America | Double | 7.3 | 1643 | ⭐⭐⭐⭐⭐ | HC | 31.9 | ⭐ | 7 | 11.50 | ⭐⭐⭐⭐⭐ | yes | |
| BIOMET GPS III | Castillo 2011 | https://pubmed.ncbi.nlm.nih.gov/21051428/ | transfer to secondary disposable | Europe | Double | 2.1 | 473 | ⭐⭐ | 27.0 | ⭐ | 6 | 2.84 | ⭐ | no | ||
| EMCYTE Genesis CS | Degen 2017 | https://pubmed.ncbi.nlm.nih.gov/28167878/ | transfer to secondary disposable | North America | Double | 5.5 | 1238 | ⭐⭐⭐⭐⭐ | HC | 26.6 | ⭐ | 6 | 7.43 | ⭐⭐⭐⭐⭐ | yes | |
| BIOMET GPS II | Kaux 2009 | https://pubmed.ncbi.nlm.nih.gov/19481375/ | transfer to secondary disposable | Europe | Double | 1.9 | 428 | ⭐⭐ | 6.0 | ⭐ | 6 | 2.57 | ⭐ | no | ||
| Vivostat.1 | Leitner 2006 | https://pubmed.ncbi.nlm.nih.gov/16907874/ | Europe | 3.0 | 681 | ⭐⭐⭐ | 92.6 | ⭐⭐⭐⭐ | yes | 5 | 3.40 | ⭐⭐ | no | |||
| Vivostat.2 | Leitner 2006 | https://pubmed.ncbi.nlm.nih.gov/16907874/ | Europe | 5.0 | 1129 | ⭐⭐⭐⭐⭐ | HC | 98.5 | ⭐⭐⭐⭐⭐ | yes | 5 | 5.64 | ⭐⭐⭐ | yes | ||
| PCCS.1 | Leitner 2006 | https://pubmed.ncbi.nlm.nih.gov/16907874/ | Europe | 4.5 | 1024 | ⭐⭐⭐⭐⭐ | HC | 38.2 | ⭐ | 7 | 7.17 | ⭐⭐⭐⭐⭐ | yes | |||
| PCCS.2 | Leitner 2006 | https://pubmed.ncbi.nlm.nih.gov/16907874/ | Europe | 2.9 | 650 | ⭐⭐⭐ | 78.0 | ⭐⭐ | 12 | 7.80 | ⭐⭐⭐⭐⭐ | yes | ||||
| PCCS.3 | Leitner 2006 | https://pubmed.ncbi.nlm.nih.gov/16907874/ | Europe | 6.5 | 1455 | ⭐⭐⭐⭐⭐ | HC | 66.7 | ⭐⭐ | 6.5 | 9.46 | ⭐⭐⭐⭐⭐ | yes | |||
| Eclipse (40 tubes) | Farah | https://www.jaad.org/article/S0190-9622(21)00088-8/fulltext | gel tube | North America | Single | 0.4 | 83 | ☆VERY LOW | ❔ | ❔ | yes | ❔ | ❔ | ❔ | yes | |
| Selphyl (3 tubes) | Farah | https://www.jaad.org/article/S0190-9622(21)00088-8/fulltext | gel tube | North America | Single | 0.3 | 76 | ☆VERY LOW | ❔ | ❔ | yes | ❔ | ❔ | ❔ | yes | |
| Emcyte (8 tubes) | Farah | https://www.jaad.org/article/S0190-9622(21)00088-8/fulltext | transfer to secondary disposable | North America | Double | 3.0 | 677 | ⭐⭐⭐ | ❔ | ❔ | yes | ❔ | ❔ | ❔ | yes | |
| PRP Medical Aesthetics | Custom PRP | https://prpclinic.ca | North America | Double | 6.0 | 1350 | ⭐⭐⭐⭐⭐ | HC | 99.4 | ⭐⭐⭐⭐⭐ | yes | 6 | 8.10 | ⭐⭐⭐⭐⭐ | yes | |
| PRP Medical Aesthetics | May 15/24 | https://prpclinic.ca | North America | Double | 11.8 | 2655 | ⭐⭐⭐⭐⭐ | HC | 99.3 | ⭐⭐⭐⭐⭐ | yes | 5.5 | 14.60 | ⭐⭐⭐⭐⭐ | yes | |
| FIDIA Hy-tissue 20 | Nov 2, 2023 | North America | Single | 2.0 | 450 | ⭐⭐ | 99.0 | ⭐⭐⭐⭐⭐ | yes | 5 | 2.25 | ⭐ | no | |||
| PuraPlas | Dec 12/23 | North America | Single | 0.7 | 158 | ☆VERY LOW | 100.0 | ⭐⭐⭐⭐⭐ | yes | 5 | 0.79 | ☆VERY LOW | no | |||
| Cellarich | Dec 12/23 | North America | Single | 0.7 | 158 | ☆VERY LOW | 100.0 | ⭐⭐⭐⭐⭐ | yes | 5 | 0.79 | ☆VERY LOW | no | |||
| Kai | Dec 22/23 | North America | Single | 0.8 | 180 | ☆VERY LOW | 97.0 | ⭐⭐⭐⭐⭐ | yes | 5 | 0.90 | ☆VERY LOW | no | |||
| ProGen 15 mL | Feb 19, 2023 | North America | Single | 1.5 | 338 | ⭐ | 99.0 | ⭐⭐⭐⭐⭐ | yes | 5.9 | 1.99 | ☆VERY LOW | no | |||
| ProGen 30 mL | Dec 18, 2023 | North America | Single | 2.7 | 608 | ⭐⭐⭐ | 95.0 | ⭐⭐⭐⭐ | yes | 5.9 | 3.58 | ⭐⭐ | no | |||
| Cellenis 22 mL | Oct 17/23, Dec 5/23 | North America | Single | 0.5 | 113 | ☆VERY LOW | 99.0 | ⭐⭐⭐⭐⭐ | yes | 12.8 | 1.44 | ☆VERY LOW | no | |||
| Cellenis 11 mL | Oct 17/23 | North America | Single | 0.7 | 158 | ☆VERY LOW | 99.0 | ⭐⭐⭐⭐⭐ | yes | 6 | 0.95 | ☆VERY LOW | no | |||
| World PRP "2x" | May 7/24 | North America | Single | 1.4 | 315 | ⭐ | 97.0 | ⭐⭐⭐⭐⭐ | yes | 16 | 5.04 | ⭐⭐⭐ | yes | |||
| World PRP "3.5x" | May 7/24 | North America | Single | 1.9 | 428 | ⭐⭐ | 97.0 | ⭐⭐⭐⭐⭐ | yes | 6 | 2.57 | ⭐ | no |
Classification and type of PRP preparation system
Although the above process is simple in theory, it may be surprising to know that there are a wide variety of different manufacturers and preparation systems in use today. Even classification systems cannot be agreed upon in the scientific literature, and quality and purity varies widely. Manufacturing terms can also be misleading, e.g. some systems claim “pure platelet-rich plasma”, but actually have very low PRP platelet counts.
In general, a commercially available centrifuge is used to concentrate platelets. It does so by separating out the RBCs and WBCs. Preparation of PRP can be done with either with a “single-spin” or “double spin system”. The type of PRP device used will affect the final PRP product and the effectiveness of the PRP therapy.
How to make single-spin PRP in 3 easy steps (plus 2 optional steps):
- Blood collection: start with a sample of the patient’s blood, usually with an anticoagulant (e.g sodium citrate or acd-a). Blood consists of plasma, with a lot of red blood cells (RBCs), white blood cells (WBCs), and platelets.
- Remove (most of) the RBCs and WBCs. Usually this is done by spinning the blood in a centrifuge.
- Optional: discard some of the plasma. Caution: you may also be removing platelets here!
- Collect the remaining plasma and call it “PRP.” Hopefully it will still have lots of platelets. Spoiler alert: this is where most PRP systems fail.
- Optional: Test the PRP for concentration and quality. Almost no one does this, but it’s the only way to be sure of the concentration and quality.
How to Double-spin PRP Preparation (a little more complicated):
- Take a blood sample. Blood is basically fluid called plasma, with a lot of cells: red blood cells (RBCs), white blood cells (WBCs), and platelets.
- Remove (most of) the RBCs and WBCs. Usually this is done by spinning the blood in a centrifuge. This is the “First Spin”.
- Second Spin: Collect and spin all the plasma in new, sterile tubes.
- You should now have tube(s) of platelet-poor plasma (PPP) with platelet pellets at the bottom.
- Remove some of the PPP and discard. Caution, PPP is not “liquid gold” as some say.
- Mix the platelet pellets into the remaining PPP and call it “PRP.” Hopefully it will still have lots of platelets, and not too many RBCs or WBCs.
- Optional: Test the PRP for concentration and quality. Almost no one does this, but it’s the only way to be sure of the concentration and quality.
Concentration levels needed for true platelet rich plasma?
This is where is starts to get tricky. The classic definition (Marx, 2001), of PRP is 1 million platelets per microliter (µL).1 There are about 50 µL in a single drop, so a drop of PRP at this concentration should have 50 million platelets. This would offer the best platelet concentration with the most growth factor release for PRP injections.
The trouble is that most platelet-rich plasma preparation systems simply can’t make PRP with such high concentration. This has been shown in multiple review publications. For example, in 2019, the Mayo Clinic looked at 33 systems. Only 10 could produce PRP at a concentration of 1 million platelets/µL. (Fadadu, 2019)3
Worse, many PRP systems tested actually actually made PPP, platelet-poor plasma. In other words, in the final concentration, they lost platelets compared to the starting blood. This would lessen the effectiveness of PRP.
Another review (Magalon, 2020), looked at results from 36 commercially available PRP kits and found that less than half of them could make PRP with a platelet concentration above 1 million/µL.2
This has led to some researchers suggesting that the definition of PRP should be relaxed to mean anything with a platelet concentration higher than blood. Whole blood starts around 150-350 thousand platelets / µL, so this is actually many times lower than a million.
For best regenerative results, PRP should have high concentration. This is especially true for procedures like PRP for Hair Loss, PRP for Knees, arthritis, other joints and orthopedic uses, wound healing,4 etc.
Best PRP: Single-Spin vs Double-Spin Centrifugation, what’s the difference?
Single-Spin PRP Pros:
- Faster to make (usually 10 minutes or less),
- Costs less
- More “pure” (less contamination with RBCs and WBCs)
- Less technical skill required for Single-Spin
Single-Spin PRP Cons:
- Much lower platelet concentration (average 291,000 /µL)
- Lower platelets = less growth factors = less results
- Dubious concentration claims by manufacturers (MPM: magical platelet multiplication)
Double-Spin PRP Advantages:
- Much higher platelet concentration (average 1.06 million/µL)
- Only verified way to get 1 million platelets / µL
- More platelets = more growth factors = better results
Double-Spin PRP Cons:
- Slower to make due to double process (up to an hour or longer),
- Costs more
- Higher technical skill required for Double-Spin PRP.
What are the ideal characteristics of PRP?
- at least 1 – 1.5 million platelets/µL in final PRP
- Pure PRP: Low percentage of RBC and WBC (<5%)
- Proper dose of platelets, eg. 5-8 billion for hair, 10+ billion for joints.
What’s the right platelet count for a PRP Treatment?
From our research and experience treating hundreds of patients, I would suggest the following:
- PRP Hair Restoration: 6 mL of PRP with concentration of 800,000-1.5 million/µL
- PRP Knee or other joint injection: 4-6 mL, concentration 1.5 million or more/µL
- PRP Under Eyes: 3-5mL total, concentration 400,000 to 700,000/µL
- PRP Vampire Facial: 4-5mL total, high concentration 800,000 – 1.5 million/µL
- PRP O-Shot: 6mL, high concentration 800,000 – 1.5 million/µL
- PRP Priapus P-Shot: 10mL, high concentration, activated, 800,000-1.5 million/µL
- PRP Acne Scar injections: Up to 5mL of high concentration, activated PRP, 800k-1.5m/µL
As you can probably tell, high concentration PRP is usually works best for almost any procedure where PRP is concerned. Keep in mind that a high total volume of blood is needed to obtain a high final platelet concentration in platelet-rich plasma.
What is platelet poor plasma, or PPP?
Platelet-poor plasma is plasma with a low concentration of platelets, usually less than 200,000 /µL. Unfortunately, sometimes PRP kits have been known to create PPP instead of PRP. This is especially true for single-spin kits (e.g. eclipse prp).
Platelet poor plasma may not be helpful. In fact, PPP may inhibit growth factor release.
There seem to be a lot of videos on YouTube and TikTok promoting PPP as “Liquid Gold” and applying, microneedling, or injecting it. Unfortunately, PPP may not be as useful as it seems, as plasma is known to have anti-angiogenic properties. In other words, it prevents the formation of new blood vessels, which are needed for the healing process. On the other hand, many growth factors in PRP work by creating blood vessels to promote tissue healing. It’s no surprise that PPP could work against PRP and lead to negative results.
Preparation of PRP: does platelet concentration really matter?
Absolutely, platelet concentration is critical. Without platelets, there are no growth factors and cytokines released, which is how PRP works to regenerate and heal tissue. One study has even shown that PRP with low platelet concentration is associated with more hair loss.5
Low concentration PRP associated with Hair Loss
Why are there so many PRP kits on the market (e.g. Eclipse, Emcyte)
PRP and regenerative medicine is still relatively new. When we first started in 2017, there were only a handful of clinics offering PRP. But as more people discover the potential benefits of PRP, the market has grown and so has the number of manufacturers. Unfortunately, many of the available kits are cheaper and only create low concentration PRP. The research shows that only a few kits are able to create high concentration PRP.
Why do so many PRP kits fail to make the right platelet concentration?
It’s a matter of cost and simplicity. Many people do not realize that all PRP kits are not the same. Only a few companies make kits that can create high concentration PRP. This has been shown in many published studies and reviews, despite what the manufacturers might claim. At our clinic, we test every PRP sample before we use it. We’ve tested thousands of PRP samples and continue to do so. We’ve even tested PRP from other clinics and found the platelet concentrations were extremely low.
Can PRP manufacturer’s claims be trusted?
Manufacturers often make exaggerated claims about the type of concentration that their kits can make. Sometimes these claims even defy simple math, claiming more platelets in their PRP than they started with in the blood sample. I wrote about this in a recent article published in the Aesthetic Surgery Journal, titled “The Emperor Has No Platelets”.6
Analyzing and testing PRP is the only way to really know the quality of your PRP.
Not all PRP is created equal. If you’ve read this far, you’re starting to understand the importance of choosing a PRP system. There are many ways of preparing PRP, but testing PRP is the only way to know the quality of the PRP you are using for your treatment. Platelet counts change from day to day, and from treatment to treatment. No kit will always make the same concentration, even from the same blood sample.
Commercially available prp kits, single spin systems:
Some examples of single-spin PRP commercial kits are: Eclipse, Regen, Selphyl, Progen, PurPlas, CellaRich
Commercially available double spin PRP systems include:
Some names of double-spin PRP Systems include: Arthrex, Harvest, Emcyte purePRP. Double spin preparation process kits will offer the highest platelet concentration.
What if the clinic doesn’t test PRP for concentration of platelets, RBCs, WBCs?
If your clinic doesn’t test PRP and you can’t find one that does, there are a few things you can do to increase the chances that you’re getting high concentration PRP:
- Ask for a small sample of your PRP to bring to our clinic – we can analyze it for you and tell you the exact concentration and purity level.
- Try to look for a double-spin centrifugation process.
- Ask the name of the system being used.
Should PRP be activated prior to injection?
Platelets are not normally “activated”, and that’s a good thing, because in the activated state, platelets form a clot, which could cause a stroke or heart attack if this occured at the wrong place and time in the body. But when there’s an injury in the body, platelets will naturally gather around the injury and activate, creating fibrin clot and releasing growth factors and cytokines which begin the healing process. Some point of care systems will mimick this activation in different ways. The most common is to add a bit of calcium solution to the mixture to start the activation process.
Different studies have looked at the value of activation of PRP. Sometimes activation seems helpful, other times it’s not as clear. Overall, concentration seems to be more important in predicting whether a PRP treatment will be successful. 7

What about anticoagulant, clots and platelet-rich fibrin, PRF?
Most PRP systems will use a bit of anticoagulant, like sodium citrate, acid citrate dextrose (e.g emcyte kits). This is to keep the blood from clotting. Some kits, like Arthrex ACP produce PRF, platelet-rich fibrin, and specfically do not use any anticoagulant. There are advantages and disadvantages to PRF. In general, Arthrex ACP PRF produces a higher concentration than most other single spin systems, but not as high as the double-spin kits e.g produced by emcyte.
Why Platelet-rich plasma preparation PRP will not work for everyone, (especially for hair loss).
PRP is not a silver bullet. It’s important to consider not only the type and quality of PRP, but also the history and specific needs of your patients. That’s why we always start with a consultation, medical history and physical exam. We may decide to order some lab tests to look for deficiencies (e.g. iron, Vitamin D, hormones), which may need addressing before considering PRP. Sometimes PRP is not the answer. There are side effects and risks with any treatment. Results cannot be guaranteed, and many of the uses of PRP are still considered experimental and under active research.
Conclusion: Look for high concentration for PRP (tested daily), and an expert provider.
In conclusion, there are a LOT of different PRP systems on the marketplace, and many of them are not what they seem. To have the best chance at success, start with a system that is known to produce high concentration, quality and purity. Ask if the clinic has a way of testing PRP for every treatment so you will know with confidence the concentration that they are using for your session. Ask whether it’s single or double-spin, PRP or PRF? What volume is used? Try to talk to a PRP expert. Please let us know if you’re interested in an expert consultation.
Academic References
- 1.Marx R. Platelet-rich plasma (PRP): what is PRP and what is not PRP? Implant Dent. 2001;10(4):225-228. doi:10.1097/00008505-200110000-00002
- 2.Magalon J, Brandin T, Francois P, et al. Technical and biological review of authorized medical devices for platelets-rich plasma preparation in the field of regenerative medicine. Platelets. 2021;32(2):200-208. doi:10.1080/09537104.2020.1832653
- 3.Fadadu P, Mazzola A, Hunter C, Davis T. Review of concentration yields in commercially available platelet-rich plasma (PRP) systems: a call for PRP standardization. Reg Anesth Pain Med. Published online April 16, 2019. doi:10.1136/rapm-2018-100356
- 4.Etulain J. Platelets in wound healing and regenerative medicine. Platelets. 2018;29(6):556-568. doi:10.1080/09537104.2018.1430357
- 5.Gentile P, Cole J, Cole M, et al. Evaluation of Not-Activated and Activated PRP in Hair Loss Treatment: Role of Growth Factor and Cytokine Concentrations Obtained by Different Collection Systems. Int J Mol Sci. 2017;18(2). doi:10.3390/ijms18020408
- 6.Yam P. The Emperor Has No Platelets: Minimal Effects in an Alopecia Split-Scalp Study Unsurprising as Platelet-Rich Plasma Was Actually Platelet-Poor. Aesthet Surg J. 2022;42(5):NP365-NP367. doi:10.1093/asj/sjab401
- 7.Trams E, Kulinski K, Kozar-Kaminska K, Pomianowski S, Kaminski R. The Clinical Use of Platelet-Rich Plasma in Knee Disorders and Surgery-A Systematic Review and Meta-Analysis. Life (Basel). 2020;10(6). doi:10.3390/life10060094